
From the book: Testosterone: A Man's Guide (click here)
Some men need to stop using testosterone or other androgens because side effects are a problem (e.g. low sperm count interferes with their goal to have children). Most physicians advise the patient to just stop testosterone without thinking about the possible consequences of the hypogonadal state after treatment cessation. Will the patient be worse off than when he started?
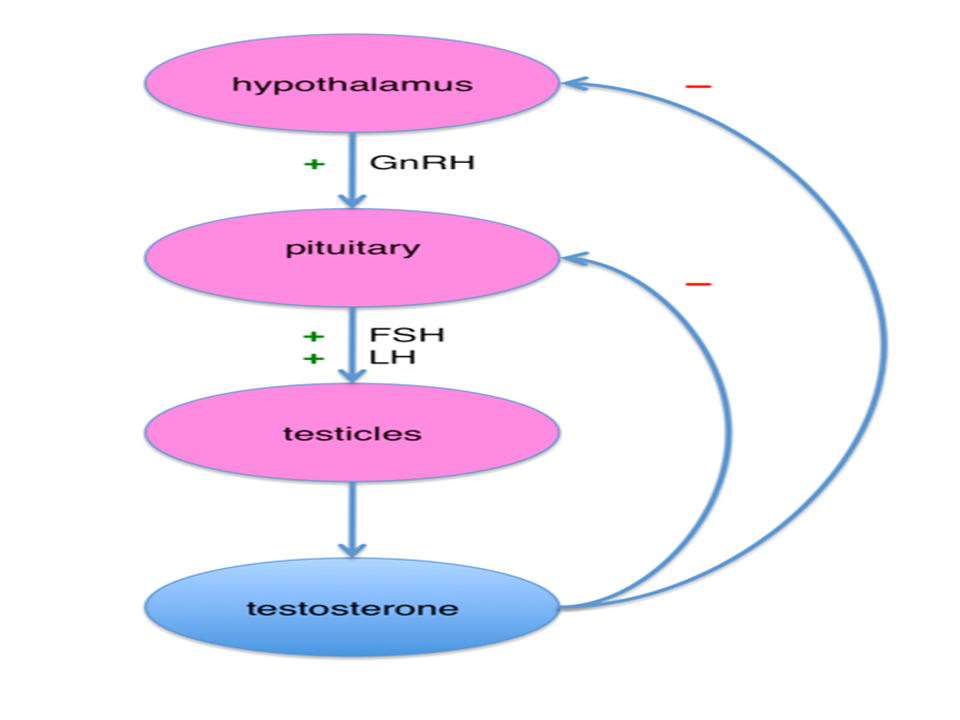
Testosterone replacement therapy and anabolic steroids can lead to HPTA (Hypothalamic-Pituitary-Testicular Axis- shown in figure below) dysfunction. Supplemental testosterone
can
inhibit the release
of
the body’s own testosterone production through negative feedback inhibition
on LH levels. This feedback
inhibition also results in suppression of FSH levels, leading
to suppression of sperm production (spermatogenesis).
Not all studies show a shutdown
of the HPTA in patients after testosterone cessation. In a study previously mentioned in the Moodiness
section, Dr. Rabkin compiled data for 42 patients
who were treated with
testosterone for 12 weeks and then randomized (double blind) to receive placebo injections for six weeks.
At week 13 (one week after their first
placebo injection and three weeks since the last active injection), mean testosterone level was 286 ng/dL. At week 15 (after 2 placebo injections), mean testosterone level was 301, and after week 17 (after 3 placebo injections), mean serum level was 324 ng/dL.
None of these values was statistically different from the mean baseline testosterone level of 308 ng/dL. These data suggest that for men who were already hypogonadal there was no further
decline in the body’s production of testosterone once testosterone therapy was discontinued after 12 weeks
of use. It is not known if longer term testosterone use would have the same results.
When high-dose
testosterone use (as in bodybuilding) is discontinued the HPTA
dysfunction that occurs when it is stopped
may be a lot more pronounced. Stopping treatment
may cause the patient to suffer all the symptoms of hypogonadism for weeks or months. Many lose a lot of the muscle mass they gained through their cycle of anabolics plus testosterone.
In some cases a specific medical protocol
is required for HPTA normalization. If you go to bodybuilding sites,
you will see Clomid and HCG
mentioned a lot for this purpose.
There is no controlled data from studies using any protocols to accelerate
the normalization of normal
testosterone production in men who have used either supplemented
physiologic (normal) or supraphysiologic (above
normal) doses of testosterone for
long periods.
For men who had normal testosterone before starting testosterone
or anabolic steroids (athletes, bodybuilders or certain people with wasting syndrome) and who want or need to stop those compounds, some physicians have attempted to jump-start testicular testosterone
production using a combination of products that have different effects on the HPTA and
estrogen receptors. One such physician
is Dr. Michael
Scally from Houston (read the interview with him: Click here ) who presented a poster at the
Lipodystrophy and Adverse Reactions in HIV conference
in San Diego in 2002 that reported
the use of a protocol
to normalize testosterone production
in HIV-positive
patients after prolonged
anabolic steroid and testosterone use for their wasting
syndrome.
The protocol
consisted of the use of HCG, clomiphene citrate, and tamoxifen (read about
each of these products
in their respective sections). Treatment
takes place over two discrete intervals. The first treatment
interval is to initiate the restoration of gonadal function.
The second interval
is to restore the hormonal pathways
among the hypothalamus, the pituitary and the
gonads. The medications are initiated simultaneously after cessation of androgens when it is expected that the body would try to start to slowly make its own testosterone. If the testosterone
ester (cypionate, enanthate,
undecanoate, Sustanon) that the patient used is known (the most common one in the United States is depo testosterone or testosterone cypionate), its half-life in the
body can be estimated
so that the
date to begin the
medical protocol can be predicted
with some accuracy to assess a time when no
pharmaceutical testosterone remains
in the body.
The protocol for HPTA normalization contains:
First 15
days:
HCG 2,500 IU (subcutaneous) once every other day;
Clomiphene citrate 50 mg orally twice a day; and
Tamoxifen 20 mg orally once a day.
A satisfactory testosterone level on day 15, typically 350 ng/mL or greater, is followed by the oral medications (no HCG) for an additional
15 days.
This protocol
has not been tested in many
patients but has shown good results in restoring HPTA in a month.
I know that this sounds like a long time but without treatment
the body’s restoration process
would take about the same length of time that somebody was using androgens. In some, HPGA function and testosterone production never returns to normal. Hopefully we will see data on approaches
like this one used in patients
who need to stop testosterone or anabolics after long term use. However,
no such studies are listed
in clinicaltrials.gov.
Most doctors
will refuse to prescribe
the protocol above since they are not familiar with it. But remember
that this protocol will likely not help most
men who had low testosterone before starting TRT anyway.
It is more
likely to be helpful to those who used testosterone and anabolics for muscle building purposes and who were not hypogonadal before starting their muscle building cycles.
More information
More information


